

ZIPSOR® (diclofenac potassium) is a prescription Non-Steroidal Anti-Inflammatory Drug (NSAID). ZIPSOR is used for relief of mild-to-moderate pain in adults (18 years of age and older).
About ZIPSOR, a non-opioid approach
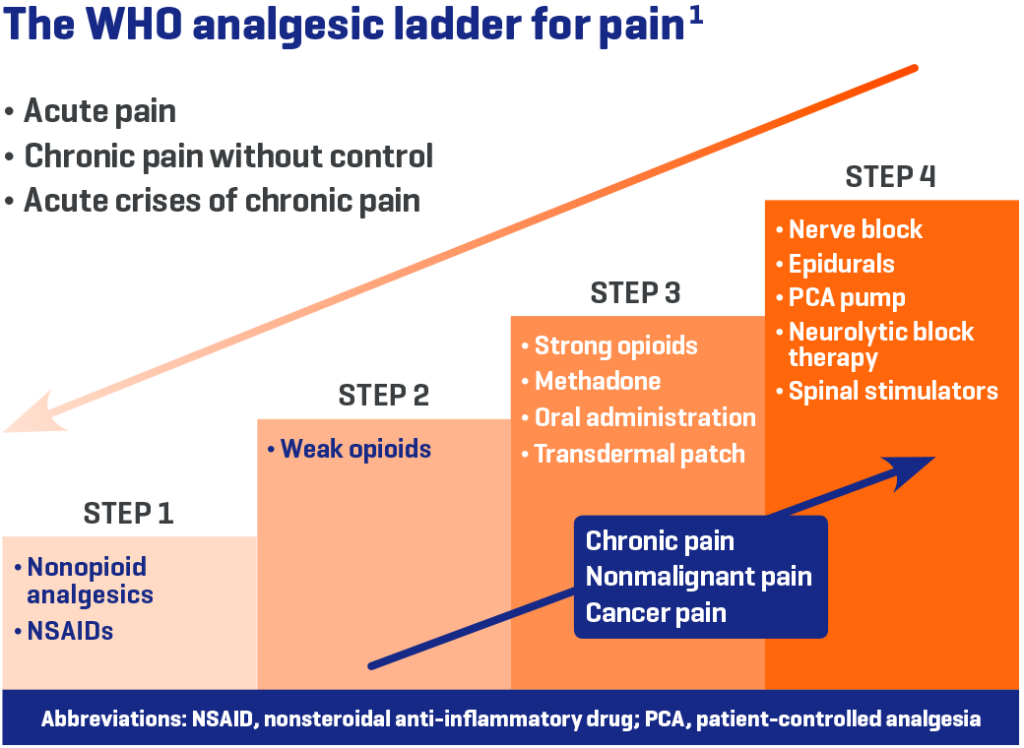
World Health Organization (WHO) recommendations for pain relief1
- Start with non-opioid analgesics, including nonsteroidal anti-inflammatory drugs (NSAIDs)
- Usage (with or without adjuvants) is suggested at every step in care
The US government’s Centers for Disease Control and Prevention (CDC) recommends that2:
- Acute pain may be managed without opioids
- Non-opioid options include NSAIDs
- Discuss with your patients about ways to relieve pain that do not involve prescription opioids
NSAIDs have been used for pain for nearly 60 years and are widely prescribed and recommended by physicians.
Why ZIPSOR?
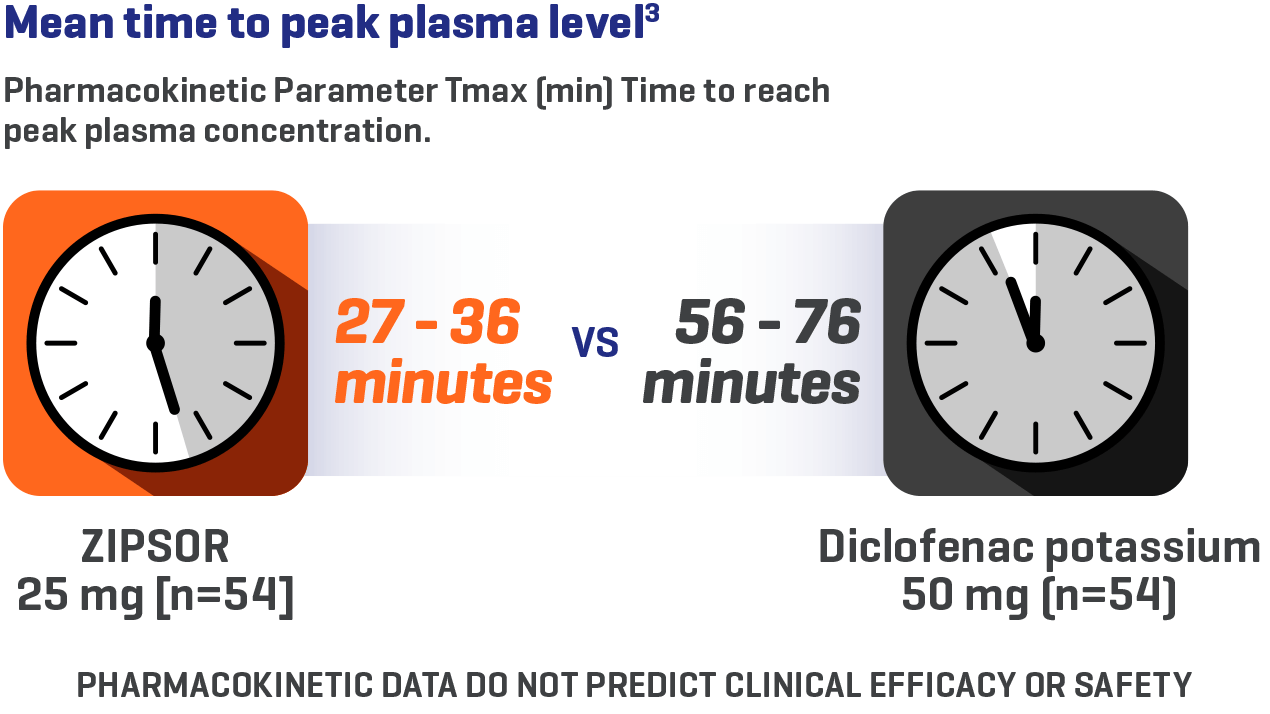
ProSorb® technology maximizes absorption3
ZIPSOR is designed for rapid, consistent absorption3*
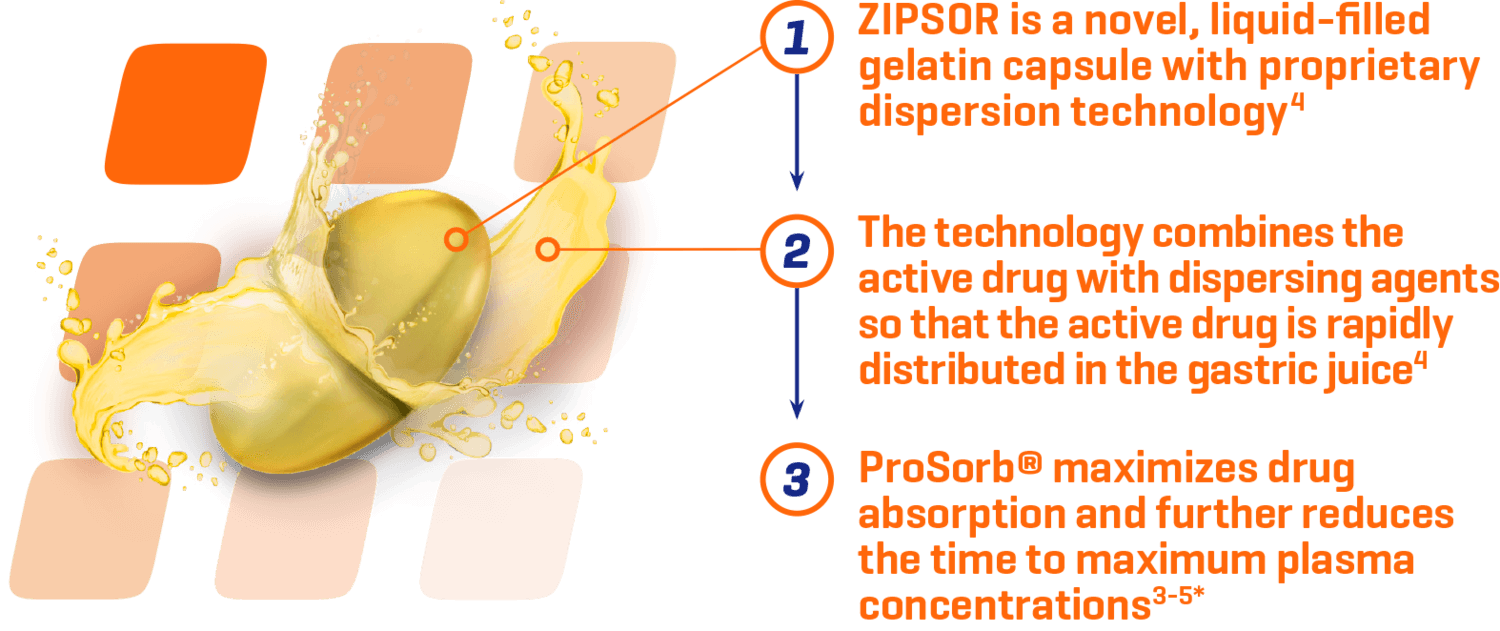
*Study conducted in healthy volunteers ≥ 18 years of age.
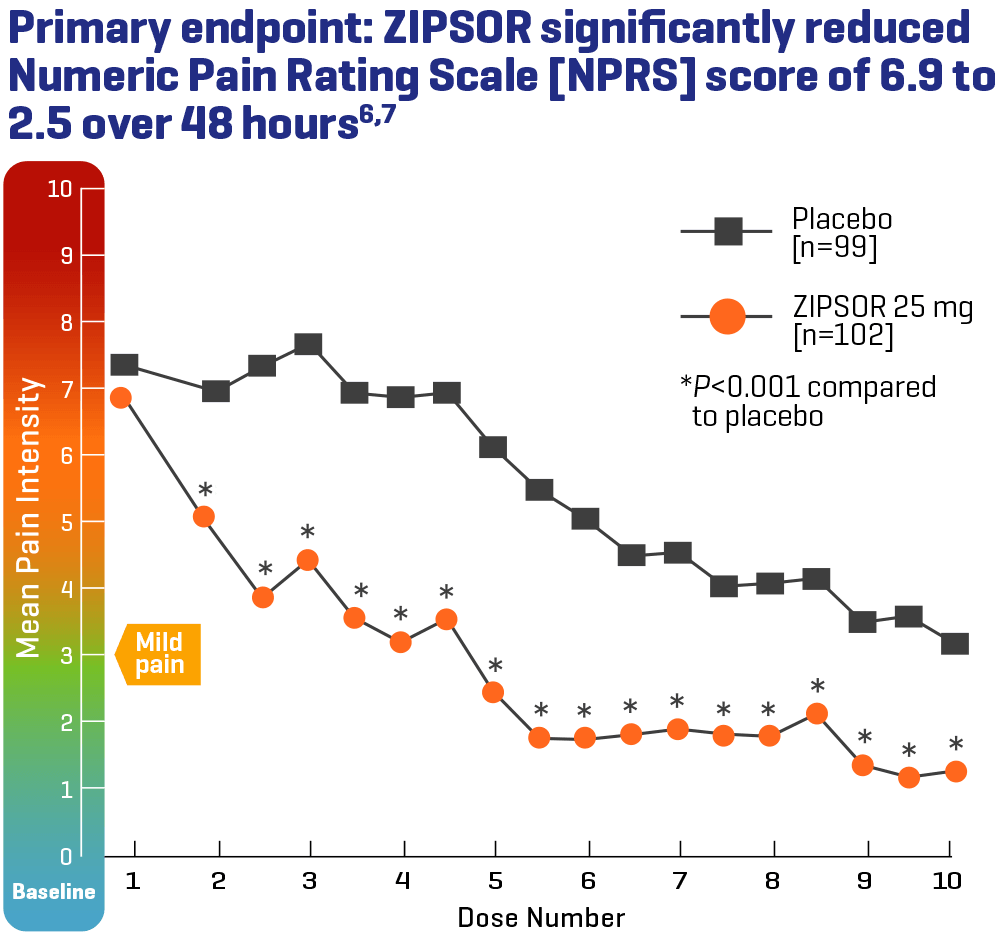
Significant pain reduction with every dose6,7
Primary endpoint: pain reduction over 48 hours after bunionectomy6,7
Bunionectomy surgery results in considerable pain and is a standard model for assessing efficacy of an acute pain medication.8
Study Design: This Phase III, randomized, double-blind, parallel-group, placebo-controlled study was conducted in a single-dose period and a multiple-dose period. Patients with a qualifying level of postsurgical pain (score ≥4 on an 11-point NPRS from 0=no pain to 10=worst possible pain) were randomly assigned to receive ZIPSOR 25 mg or placebo soft gelatin capsules in a 1:1 ratio.7
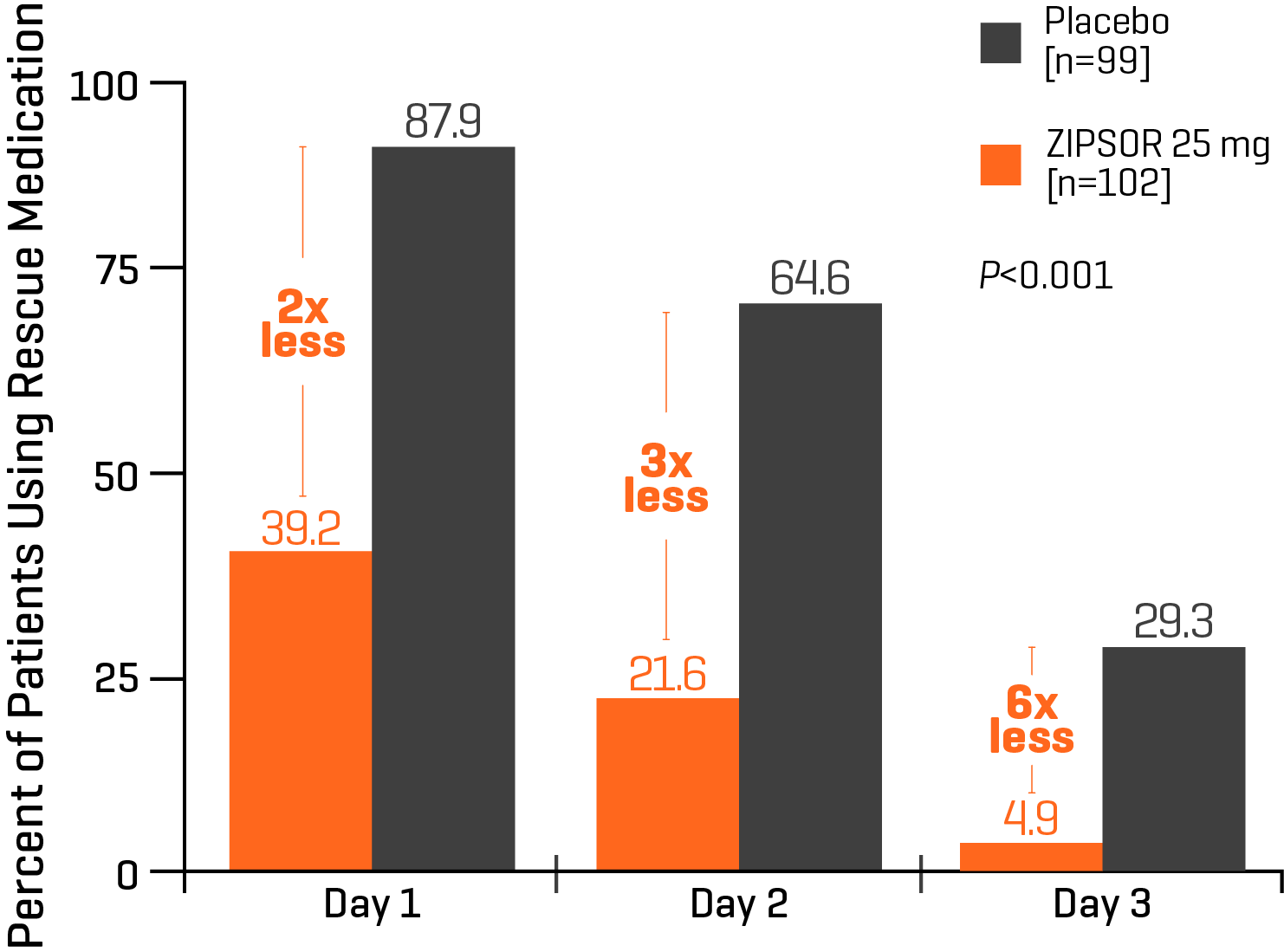
Use of rescue medication (1-2 hydrocodone/acetaminophen tablets) during the inpatient 48-hour multiple-dose period after bunionectomy in patients who received ZIPSOR 25 mg or placebo. Day 3 was not a full day, and the data reflect use of rescue medication only up to the time of discharge.7

Your patients can save on ZIPSOR
Your patients can save money on ZIPSOR by downloading a copay card.*
*Terms and conditions may apply. View savings card for full terms and conditions.
Please see Important Safety Information and full Prescribing Information, including BOXED WARNING.
INDICATION
ZIPSOR® (diclofenac potassium) Liquid Filled Capsules are indicated for relief of mild to moderate acute pain in adults (18 years of age or older).
IMPORTANT SAFETY INFORMATION
DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of ZIPSOR and other treatment options before deciding to use ZIPSOR. Use the lowest effective dosage for the shortest duration consistent with individual patient treatment goals.
Non-Interchangeability with Other Formulations of Diclofenac
Different dose strengths and formulations of oral diclofenac are not interchangeable. This difference should be taken into consideration when changing strengths or formulations. The only approved dosing regimen for ZIPSOR is 25 mg four times a day.
CONTRAINDICATIONS
ZIPSOR is contraindicated in the following patients:
- Known hypersensitivity (e.g., anaphylactic reactions and serious skin reactions) to diclofenac or any components of the drug product
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs. Severe, sometimes fatal, anaphylactic reactions to NSAIDs have been reported in such patients
- In the setting of coronary artery bypass graft (CABG) surgery
- ZIPSOR contains gelatin and is contraindicated in patients with known hypersensitivity to bovine protein
WARNINGS AND PRECAUTIONS
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Risk
- Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use.
- ZIPSOR is contraindicated in the setting of coronary artery bypass graft (CABG) surgery.
Gastrointestinal Bleeding, Ulceration, and Perforation
- NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events, including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events.
Cardiovascular Thrombotic Events
Clinical trials of several COX-2 selective and nonselective NSAIDs of up to three years duration have shown an increased risk of serious cardiovascular (CV) thrombotic events, including myocardial infarction (MI) and stroke, which can be fatal.
To minimize the potential risk for an adverse CV event in NSAID-treated patients, use the lowest effective dose for the shortest duration possible. Physicians and patients should remain alert for the development of such events, throughout the entire treatment course, even in the absence of previous CV symptoms. Patients should be informed about the symptoms of serious CV events and the steps to take if they occur.
Post-MI Patients
Avoid the use of ZIPSOR in patients with a recent MI unless the benefits are expected to outweigh the risk of recurrent CV thrombotic events. If ZIPSOR is used in patients with a recent MI, monitor patients for signs of cardiac ischemia.
Gastrointestinal Bleeding, Ulceration, and Perforation
NSAIDs, including diclofenac, cause serious gastrointestinal (GI) adverse events including inflammation, bleeding, ulceration, and perforation of the esophagus, stomach, small intestine, or large intestine, which can be fatal. These serious adverse events can occur at any time, with or without warning symptoms, in patients treated with NSAIDs. Only one in five patients who develop a serious upper GI adverse event on NSAID therapy is symptomatic.
Hepatotoxicity
Inform patients of the warning signs and symptoms of hepatotoxicity (e.g., nausea, fatigue, lethargy, diarrhea, pruritus, jaundice, right upper quadrant tenderness, and “flu-like” symptoms). If clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur (e.g., eosinophilia, rash, etc.), discontinue ZIPSOR immediately, and perform a clinical evaluation of the patient. Exercise caution when prescribing ZIPSOR with concomitant drugs that are known to be potentially hepatotoxic (e.g., acetaminophen, antibiotics, antiepileptics).
To minimize the potential risk for an adverse liver-related event in patients treated with ZIPSOR, use the lowest effective dose for the shortest duration possible.
Hypertension
NSAIDs, including ZIPSOR, can lead to new onset of hypertension or worsening of preexisting hypertension, either of which may contribute to the increased incidence of CV events. Patients taking angiotensin converting enzyme (ACE) inhibitors, thiazide diuretics, or loop diuretics may have impaired response to these therapies when taking NSAIDs.
Monitor blood pressure (BP) during the initiation of NSAID treatment and throughout the course of therapy.
Heart Failure and Edema
A meta-analysis of randomized controlled trials demonstrated an approximately two-fold increase in hospitalizations for heart failure in COX-2 selective-treated patients and nonselective NSAID-treated patients compared to placebo-treated patients. In a Danish National Registry study of patients with heart failure, NSAID use increased the risk of MI, hospitalization for heart failure, and death.
Avoid the use of ZIPSOR in patients with severe heart failure unless the benefits are expected to outweigh the risk of worsening heart failure. If ZIPSOR is used in patients with severe heart failure, monitor patients for signs of worsening heart failure.
Renal Toxicity and Hyperkalemia
Renal Toxicity
Renal Toxicity: Monitor renal function in patients with renal or hepatic impairment, heart failure, dehydration, or hypovolemia. Avoid use of ZIPSOR in patients with advanced renal disease unless benefits are expected to outweigh risk of worsening renal function.
Anaphylactic Reactions
Diclofenac has been associated with anaphylactic reactions in patients with and without known hypersensitivity to diclofenac and in patients with aspirin-sensitive asthma.
Exacerbation of Asthma Related to Aspirin Sensitivity
ZIPSOR is contraindicated in patients with aspirin-sensitive asthma. Monitor patients with preexisting asthma (without aspirin sensitivity).
Serious Skin Reactions
NSAIDs, including diclofenac, can cause serious skin adverse events such as exfoliative dermatitis, Stevens-Johnson Syndrome, and toxic epidermal necrolysis, which can be fatal. These serious events can occur without warning. Inform patients about the signs and symptoms of serious skin reactions, and to discontinue the use of ZIPSOR at the first appearance of skin rash or any other sign of hypersensitivity. ZIPSOR is contraindicated in patients with previous serious skin reactions to NSAIDs.
Hematologic Toxicity
Anemia has occurred in NSAID-treated patients. If a patient treated with ZIPSOR has any signs or symptoms of anemia, monitor hemoglobin or hematocrit.
NSAIDs, including ZIPSOR, may increase the risk of bleeding events. Co-morbid conditions such as coagulation disorders, concomitant use of warfarin, other anticoagulants, antiplatelet agents (e.g., aspirin), serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs) may increase this risk. Monitor these patients for signs of bleeding.
ADVERSE REACTIONS
The most common adverse reactions reported in ZIPSOR clinical trials (≥1% and greater than placebo) were abdominal pain, constipation, somnolence, and increased sweating.
DRUG INTERACTIONS
Drugs that Interfere with Hemostasis (e.g. warfarin, aspirin, SSRIs/SNRIs)
Monitor patients for bleeding who are concomitantly taking ZIPSOR with drugs that interfere with hemostasis. Concomitant use of ZIPSOR and analgesic doses of aspirin is not generally recommended.
ACE Inhibitors, Angiotensin Receptor Blockers (ARB), or Beta-Blockers
Concomitant use with ZIPSOR may diminish the antihypertensive effect of these drugs. Monitor blood pressure.
ACE Inhibitors and ARBs
Concomitant use with ZIPSOR in elderly, volume depleted, or those with renal impairment may result in deterioration of renal function. In such high-risk patients, monitor for signs of worsening renal function.
Diuretics
NSAIDs can reduce natriuretic effect of furosemide and thiazide diuretics. Monitor patients to assure diuretic efficacy including antihypertensive effects.
Digoxin
Concomitant use with ZIPSOR can increase serum concentration and prolong half-life of digoxin. Monitor serum digoxin levels.
Please see full Prescribing Information for complete information about Drug Interactions.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category C prior to 30 weeks gestation; Category D starting 30 weeks gestation.
Use of NSAIDs during the third trimester of pregnancy increases the risk of premature closure of the fetal ductus arteriosus. Avoid use of NSAIDs in pregnant women starting at 30 weeks gestation.
Infertility
NSAIDs are associated with reversible infertility. Consider withdrawal of ZIPSOR in women who have difficulties conceiving.
Lactation
Risk Summary
It is not known whether this drug is excreted in human milk; however, there is a case report in the literature indicating that diclofenac can be detected at low levels in breast milk.
Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from ZIPSOR, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
The safety and effectiveness of ZIPSOR in pediatric patients has not been established.
Geriatric Use
Elderly patients, compared to younger patients, are at greater risk for NSAID-associated serious cardiovascular, gastrointestinal, and/or renal adverse reactions. If the anticipated benefit for the elderly patient outweighs these potential risks, start dosing at the low end of the dosing range, and monitor patients for adverse effects.
OVERDOSAGE
Symptoms following acute NSAID overdosages have been typically limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which have been generally reversible with supportive care. Gastrointestinal bleeding has occurred. Hypertension, acute renal failure, respiratory depression, and coma have occurred, but were rare.
Please see full Prescribing Information and Medication Guide for more information about ZIPSOR.
REFERENCES: 1. Vargas-Schaffer G. Is the WHO analgesic ladder still valid? Twenty-four years of experience. Can Fam Physician. 2010;56(6):514-517. 2. Centers for Disease Control and Prevention. Opioids for acute pain: what you need to know. https://www.cdc.gov/drugoverdose/pdf/patients/Opioids-for-Acute-Pain-a.pdf. Accessed October 9, 2018. 3. Lissy M, Scallion R, Stiff DD, Moore K. Pharmacokinetic comparison of an oral diclofenac potassium liquid-filled soft gelatin capsule with a diclofenac potassium tablet. Expert Opin Pharmacother. 2010;11(5):701-708. 4. Cole BE. Treating mild to moderate acute pain with oral diclofenac potassium liquid-filled capsules: rapid absorption with ProSorb dispersion technology. Pain Medicine News. 2011;March:1-8. 5. Altman R, Bosch B, Brune K, Patrignani P, Young C. Advances in NSAID development: evolution of diclofenac products using pharmaceutical technology. Drugs. 2015;75(8):859-877. 6. ZIPSOR [package insert]. Lake Forest, IL: Assertio Therapeutics, Inc.; 2025. 7. Riff DS, Duckor S, Gottlieb I, et al. Diclofenac potassium liquid-filled soft gelatin capsules in the management of patients with postbunionectomy pain: a Phase III, multicenter, randomized, double-blind, placebo-controlled study conducted over 5 days. Clin Ther. 2009;31(10):2072-2085. 8. Singla NK, Desjardins PJ, Chang PD. A comparison of the clinical and experimental characteristics of four acute surgical pain models: dental extraction, bunionectomy, joint replacement, and soft tissue surgery. Pain. 2014;155(3):441-456.
INDICATION
ZIPSOR® (diclofenac potassium) Liquid Filled Capsules are indicated for relief of mild to moderate acute pain in adults (18 years of age or older).
IMPORTANT SAFETY INFORMATION
DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of ZIPSOR and other treatment options before deciding to use ZIPSOR. Use the lowest effective dosage for the shortest duration consistent with individual patient treatment goals.
Non-Interchangeability with Other Formulations of Diclofenac
Different dose strengths and formulations of oral diclofenac are not interchangeable. This difference should be taken into consideration when changing strengths or formulations. The only approved dosing regimen for ZIPSOR is 25 mg four times a day.
CONTRAINDICATIONS
ZIPSOR is contraindicated in the following patients:
- Known hypersensitivity (e.g., anaphylactic reactions and serious skin reactions) to diclofenac or any components of the drug product
- History of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs. Severe, sometimes fatal, anaphylactic reactions to NSAIDs have been reported in such patients
- In the setting of coronary artery bypass graft (CABG) surgery
- ZIPSOR contains gelatin and is contraindicated in patients with known hypersensitivity to bovine protein
WARNINGS AND PRECAUTIONS
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Risk
- Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use.
- ZIPSOR is contraindicated in the setting of coronary artery bypass graft (CABG) surgery.
Gastrointestinal Bleeding, Ulceration, and Perforation
- NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events, including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events.
Cardiovascular Thrombotic Events
Clinical trials of several COX-2 selective and nonselective NSAIDs of up to three years duration have shown an increased risk of serious cardiovascular (CV) thrombotic events, including myocardial infarction (MI) and stroke, which can be fatal.
To minimize the potential risk for an adverse CV event in NSAID-treated patients, use the lowest effective dose for the shortest duration possible. Physicians and patients should remain alert for the development of such events, throughout the entire treatment course, even in the absence of previous CV symptoms. Patients should be informed about the symptoms of serious CV events and the steps to take if they occur.
Post-MI Patients
Avoid the use of ZIPSOR in patients with a recent MI unless the benefits are expected to outweigh the risk of recurrent CV thrombotic events. If ZIPSOR is used in patients with a recent MI, monitor patients for signs of cardiac ischemia.
Gastrointestinal Bleeding, Ulceration, and Perforation
NSAIDs, including diclofenac, cause serious gastrointestinal (GI) adverse events including inflammation, bleeding, ulceration, and perforation of the esophagus, stomach, small intestine, or large intestine, which can be fatal. These serious adverse events can occur at any time, with or without warning symptoms, in patients treated with NSAIDs. Only one in five patients who develop a serious upper GI adverse event on NSAID therapy is symptomatic.
Hepatotoxicity
Inform patients of the warning signs and symptoms of hepatotoxicity (e.g., nausea, fatigue, lethargy, diarrhea, pruritus, jaundice, right upper quadrant tenderness, and “flu-like” symptoms). If clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur (e.g., eosinophilia, rash, etc.), discontinue ZIPSOR immediately, and perform a clinical evaluation of the patient. Exercise caution when prescribing ZIPSOR with concomitant drugs that are known to be potentially hepatotoxic (e.g., acetaminophen, antibiotics, antiepileptics).
To minimize the potential risk for an adverse liver-related event in patients treated with ZIPSOR, use the lowest effective dose for the shortest duration possible.
Hypertension
NSAIDs, including ZIPSOR, can lead to new onset of hypertension or worsening of preexisting hypertension, either of which may contribute to the increased incidence of CV events. Patients taking angiotensin converting enzyme (ACE) inhibitors, thiazide diuretics, or loop diuretics may have impaired response to these therapies when taking NSAIDs.
Monitor blood pressure (BP) during the initiation of NSAID treatment and throughout the course of therapy.
Heart Failure and Edema
A meta-analysis of randomized controlled trials demonstrated an approximately two-fold increase in hospitalizations for heart failure in COX-2 selective-treated patients and nonselective NSAID-treated patients compared to placebo-treated patients. In a Danish National Registry study of patients with heart failure, NSAID use increased the risk of MI, hospitalization for heart failure, and death.
Avoid the use of ZIPSOR in patients with severe heart failure unless the benefits are expected to outweigh the risk of worsening heart failure. If ZIPSOR is used in patients with severe heart failure, monitor patients for signs of worsening heart failure.
Renal Toxicity and Hyperkalemia
Renal Toxicity
Renal Toxicity: Monitor renal function in patients with renal or hepatic impairment, heart failure, dehydration, or hypovolemia. Avoid use of ZIPSOR in patients with advanced renal disease unless benefits are expected to outweigh risk of worsening renal function.
Anaphylactic Reactions
Diclofenac has been associated with anaphylactic reactions in patients with and without known hypersensitivity to diclofenac and in patients with aspirin-sensitive asthma.
Exacerbation of Asthma Related to Aspirin Sensitivity
ZIPSOR is contraindicated in patients with aspirin-sensitive asthma. Monitor patients with preexisting asthma (without aspirin sensitivity).
Serious Skin Reactions
NSAIDs, including diclofenac, can cause serious skin adverse events such as exfoliative dermatitis, Stevens-Johnson Syndrome, and toxic epidermal necrolysis, which can be fatal. These serious events can occur without warning. Inform patients about the signs and symptoms of serious skin reactions, and to discontinue the use of ZIPSOR at the first appearance of skin rash or any other sign of hypersensitivity. ZIPSOR is contraindicated in patients with previous serious skin reactions to NSAIDs.
Hematologic Toxicity
Anemia has occurred in NSAID-treated patients. If a patient treated with ZIPSOR has any signs or symptoms of anemia, monitor hemoglobin or hematocrit.
NSAIDs, including ZIPSOR, may increase the risk of bleeding events. Co-morbid conditions such as coagulation disorders, concomitant use of warfarin, other anticoagulants, antiplatelet agents (e.g., aspirin), serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs) may increase this risk. Monitor these patients for signs of bleeding.
ADVERSE REACTIONS
The most common adverse reactions reported in ZIPSOR clinical trials (≥1% and greater than placebo) were abdominal pain, constipation, somnolence, and increased sweating.
DRUG INTERACTIONS
Drugs that Interfere with Hemostasis (e.g. warfarin, aspirin, SSRIs/SNRIs)
Monitor patients for bleeding who are concomitantly taking ZIPSOR with drugs that interfere with hemostasis. Concomitant use of ZIPSOR and analgesic doses of aspirin is not generally recommended.
ACE Inhibitors, Angiotensin Receptor Blockers (ARB), or Beta-Blockers
Concomitant use with ZIPSOR may diminish the antihypertensive effect of these drugs. Monitor blood pressure.
ACE Inhibitors and ARBs
Concomitant use with ZIPSOR in elderly, volume depleted, or those with renal impairment may result in deterioration of renal function. In such high-risk patients, monitor for signs of worsening renal function.
Diuretics
NSAIDs can reduce natriuretic effect of furosemide and thiazide diuretics. Monitor patients to assure diuretic efficacy including antihypertensive effects.
Digoxin
Concomitant use with ZIPSOR can increase serum concentration and prolong half-life of digoxin. Monitor serum digoxin levels.
Please see full Prescribing Information for complete information about Drug Interactions.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category C prior to 30 weeks gestation; Category D starting 30 weeks gestation.
Use of NSAIDs during the third trimester of pregnancy increases the risk of premature closure of the fetal ductus arteriosus. Avoid use of NSAIDs in pregnant women starting at 30 weeks gestation.
Infertility
NSAIDs are associated with reversible infertility. Consider withdrawal of ZIPSOR in women who have difficulties conceiving.
Lactation
Risk Summary
It is not known whether this drug is excreted in human milk; however, there is a case report in the literature indicating that diclofenac can be detected at low levels in breast milk.
Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from ZIPSOR, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
The safety and effectiveness of ZIPSOR in pediatric patients has not been established.
Geriatric Use
Elderly patients, compared to younger patients, are at greater risk for NSAID-associated serious cardiovascular, gastrointestinal, and/or renal adverse reactions. If the anticipated benefit for the elderly patient outweighs these potential risks, start dosing at the low end of the dosing range, and monitor patients for adverse effects.
OVERDOSAGE
Symptoms following acute NSAID overdosages have been typically limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which have been generally reversible with supportive care. Gastrointestinal bleeding has occurred. Hypertension, acute renal failure, respiratory depression, and coma have occurred, but were rare.
REFERENCES: 1. Centers for Disease Control and Prevention. Opioids for acute pain: what you need to know. https://www.cdc.gov/drugoverdose/pdf/patients/Opioids-for-Acute-Pain-a.pdf. Accessed October 9, 2018. 2. Lissy
M, Scallion R, Stiff DD, Moore K. Pharmacokinetic comparison of an oral diclofenac potassium liquid-filled soft gelatin capsule with a diclofenac potassium tablet. Expert Opin Pharmacother. 2010;11(5):701-708. 3. Cole
BE. Treating mild to moderate acute pain with oral diclofenac potassium liquid-filled capsules: rapid absorption with ProSorb dispersion technology. Pain Medicine News. 2011;March:1-8. 4. Riff
DS, Duckor S, Gottlieb I, et al. Diclofenac potassium liquid-filled soft gelatin capsules in the management of patients with postbunionectomy pain: a Phase III, multicenter, randomized, double-blind, placebo-controlled study conducted over 5 days. Clin Ther. 2009;31(10):2072-2085. 5. ZIPSOR.
[package insert]. Lake Forest, IL: Assertio Therapeutics, Inc.; 2016.